

Photo credits: IRC/Jessica Wanless
For newborn care being provided at the primary care level, in addition to the actions described under Section 3.3, program managers and health care providers should consider implementing the following:
3.4.1 Antenatal care
- Diagnose and promptly treat urinary tract infections, STIabbreviation, other maternal illnesses and complications like pre-eclampsia and diabetes, where feasibleinfo otherwise refer to higher facilities.
- Provide asymptomatic bacteriuria screening and treatment.
- Provide folate, iron and other micro-nutrient supplements as needed.
For pre-term and/or LBW babies
For women who have completed less than 34 weeks of pregnancy and have one of the five conditions associated with preterm birth (i.e., preterm labor, premature rupture of the membranes, antepartum haemorrhage, multiple pregnancy, severe pre-eclampsia), refer to a hospital for further monitoring. ACSabbreviation should only be administered as per WHOabbreviation guidelines (see Section 3.6).
3.4.2 Intrapartum and essential newborn care
- Provide respectful, supportive care to the woman: maintain privacy; encourage her to have a birth companion, choose her birthing position, to move around and drink fluids; ensure that all information is communicated clearly to her.
- If the primary care facility is equipped to do normal deliveries, monitor labor with the use of the partogram, documenting critical maternal and fetal statistics (e.g., cervical dilation, fetal heart rate, progress of labor) every 30 minutes during the 1st of stage of labor and more frequently during the second stage of labor.
- If maternal or fetal distress is recognized, identify transport and use established referral systems to get the woman to a health facility that has basic or comprehensive emergency obstetric and newborn care (BEmONC or CEmONC).
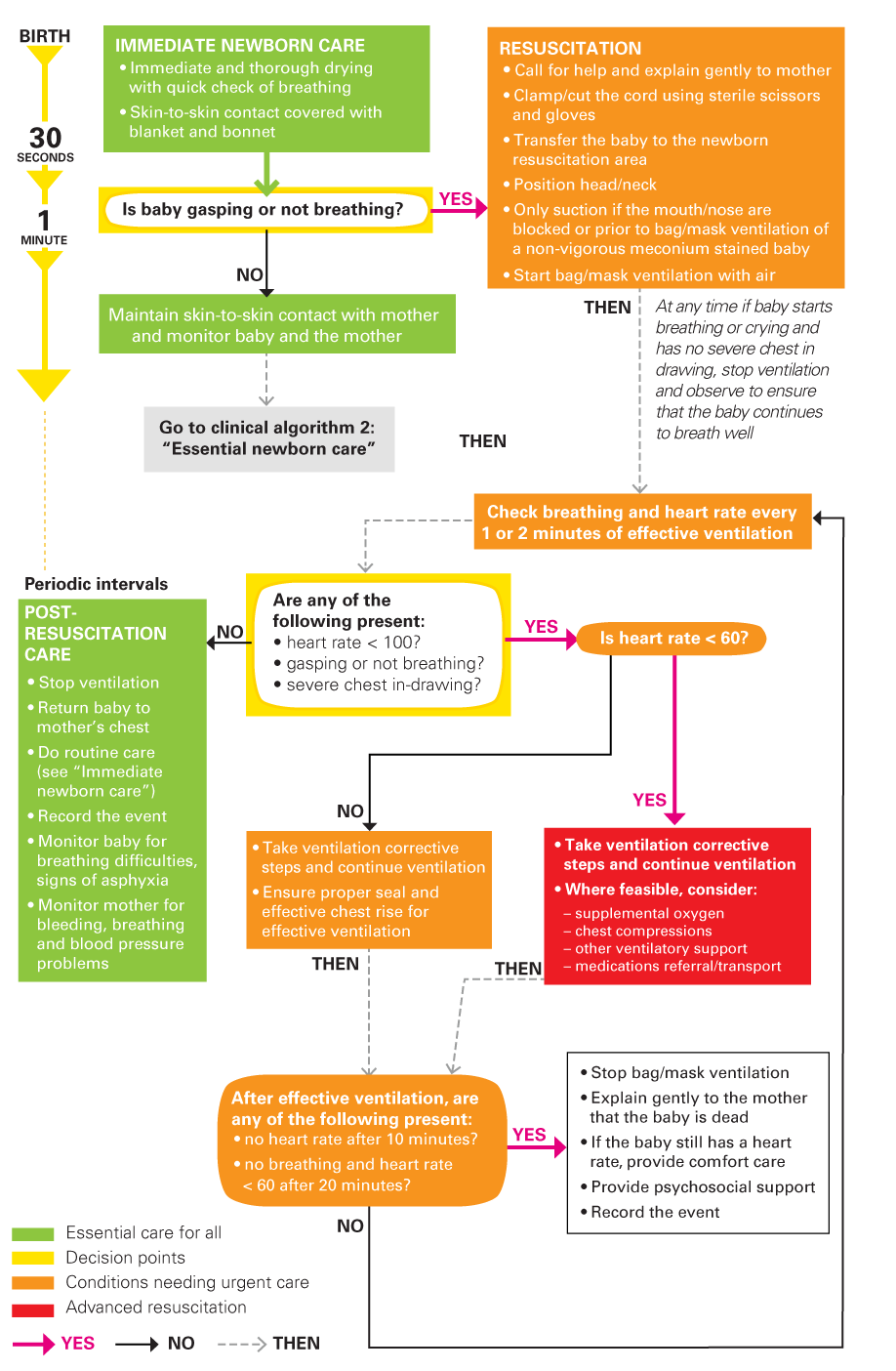
- For newborns who do not start breathing on their own after tactile stimulation within one minute after birth, provide basic newborn resuscitation (Figure 3.3).
- Administer antibiotics to newborns who are born with the following risks (even if no signs of clinical infection):
- The mother has or had a uterine infection or fever any time from the onset of labor to three days after birth;
- The mother had premature rupture of membranes for more than 18 hours before birth and/or foul smelling amniotic fluid.
- Duration of antibiotics should be at least 48 hours if laboratory studies and exam are normal. Longer treatment duration is required if laboratory results suggest infection or if clinical signs are present.
- Encourage health staff to review maternal records to assess the need for antibiotics and other newborn health interventions.
In case of intrapartum complications during birth
- Follow the Newborn Resuscitation Flowchart (Figure 3.3) for immediate action steps at birth.
- Assess adequacy of ventilation by observing chest rise and fall. If normal breathing has not started, use the bag and mask for oxygen administration and monitor oxygen levels with a battery operated pulse oximeter with probes for neonates.
- Have a mucus trap (e.g., Penguin Suction Device) available for suction or a suction machine.
- If continued oxygen administration is needed and equipment for providing oxygen monitoring saturation is available, use nasal prongs.
3.4.3 Postnatal care
During the immediate postnatal period (within the first hour of birth)
- Assess breastfeeding and provide support where needed.
- Provide birth certificate or record of birth card to the mother or family, in accordance with national practice.
For pre-term and/or LBWabbreviation babies
- Ensure availability of heel lancets and rapid blood sugar testing sticks.
- Provide extra thermal care for small babies through KMCabbreviation (Box 3.2).
- Employ strict infection-prevention measures through strict hand washing (Figure 3.2), ensuring a clean environment and avoiding sharing of incubators.
- Provide feeding support (e.g., cup and spoon, nasogastric tube) if the baby is unable to breastfeed.
For babies exhibiting danger signs or indicators of neonatal infections
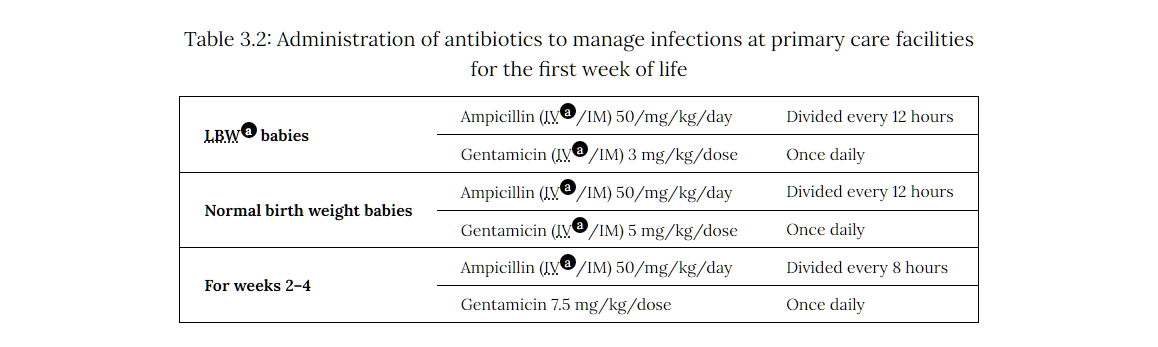
- Immediately administer an initial dose of antibiotics, provide respiratory support or anti-convulsant (phenobarbital) if needed, and refer mother and baby to the nearest hospital for advanced care.[1][2] See Table 3.2 for further guidance.
- As good practice, ensure dosing tables for gentamicin and ampicillin by weight band are posted in the labor ward in settings where health workers have difficulty calculating dosages.
|
LBWabbreviation babies |
Ampicillin (IVabbreviation/IM) 50/mg/kg/day |
Divided every 12 hours |
|---|---|---|
|
Gentamicin (IVabbreviation/IM) 3 mg/kg/dose |
Once daily | |
| Normal birth weight babies |
Ampicillin (IVabbreviation/IM) 50/mg/kg/day |
Divided every 12 hours |
|
Gentamicin (IVabbreviation/IM) 5 mg/kg/dose |
Once daily | |
| For weeks 2–4 |
Ampicillin (IVabbreviation/IM) 50/mg/kg/day |
Divided every 8 hours |
| Gentamicin 7.5 mg/kg/dose | Once daily |
{kind=link}
For medical supplies needed at the facility level see Box 3.11.
Box 3.11: Checklist of medical supplies needed at the facility level and/or hospital level
- two sizes of bag and mask (for term and preterm babies) and simple suction for resuscitation
- digital infant weighing scale
- digital infant thermometer
- mobile examination lamp
- syringes (2, 5, 10 cc) and needles (16,18)
- alcohol swabs
- phototherapy
- oxygen concentrator plus consistent oxygen source
- nasal prong
- pulse oximetry
Additional/optional items include breast pump (battery powered or manual), phototherapy lamp and fluorescent tubes. The Clinic/Primary Care Facility Newborn Kit contains these and other supplies; see Annex 5.
{kind=link}
During the first week after birth (second hour following birth up to seven days)
- Perform a complete physical examination following the first hour.
- Prior to discharge, assess mothers and their new babies for danger signs of serious infections and for other problems (e.g., congenital malformations, such as cleft palate).
- Regularly assess all postpartum women for vaginal bleeding, uterine contraction, fundal height, temperature and heart rate (pulse) routinely during the first 24 hours starting from the first hour after birth.
- Where possible, keep the healthy mother and baby together in the facility to receive postnatal care for at least 24 hours. Otherwise, coordinate with field staff to organize a first home visit from a trained health worker within 24 hours after birth.
- Organise, at minimum, two more home visits for postnatal care to take place between 48-72 hours and between day 7-14 after birth. Where home visits are not feasible, instruct women to return to the facility between these two time periods for two postnatal check-ups. WHOabbreviation also recommends a postnatal contact during week 6 after birth.
- Emphasize the importance of postnatal contacts, even if everything is going well.
- Advise women to return immediately to the facility if they notice any danger signs (Box 3.3).
- For babies born to positive mothers, initiate antiretroviral therapy (ART) in accordance with relevant protocols.info
For pre-term and/or LBWabbreviation babies
- Measure the newborn’s body temperature every four hours and observe and monitor other newborn vital signs for a minimum of 24 hours.
- Weigh the newborn at least once per day.
- Monitor for signs of jaundice (Box 3.10).
- Continue STSabbreviation or KMCabbreviation (Box 3.2) with careful monitoring of feeding, weight gain and signs of illness, especially infection.
- Continue providing ENCabbreviation and feed breast milk every 2 to 3 hours for about 20 minutes per session until the baby is tolerating feeds, is alert and has no signs of hypoglycemia.[3] Many preterm babies will not feed on demand and should be woken up to feed on schedule to ensure they are eating enough in order to gain weight and prevent hypoglycemia.
- For newborns who are having difficulty breastfeeding, ensure mothers are comfortable hand-expressing breast milk; emphasize the importance of hand washing before expressing breast milk and of keeping all feeding cups and utensils clean.
- Provide antibiotic prophylaxis for newborns at risk of infection due to pPROMabbreviation or meconium aspiration during birth [intravenous (IV)/intramuscular (IM) ampicillin powder for injection 500 mg vial (250mg/ml); IV/IM gentamicin, 40mg/ml (20mg/ml, if available)].